The aspirate smear is hypercellular and shows loosely cohesive sheets of epithelioid cells with abundant fibrillary cytoplasm and indistinct cell borders (Figures 1 and 2). The nuclei are ovoid with smooth nuclear contours and variably prominent nucleoli. Moderate nuclear pleomorphism is present. In several areas, endothelial cells course through the sheets of epithelioid cells (Figures 1, 2, and 3). A mixed inflammatory infiltrate is associated with the epithelioid cells (Figure 2). A concurrent core biopsy specimen highlights the cytologic similarities and differences between benign hepatocytes (Figure 4) and the lesional epithelioid cells (Figure 5).
The cytomorphologic differential diagnosis of epithelioid angiomyolipoma includes hepatocellular carcinoma (HCC) and clear cell renal cell carcinoma (RCC). In cases where the adipose component of an angiomyolipoma is absent or not prominent, the morphologic distinction between these tumors can be difficult. All three tumors are vascular and may show “transgressing” endothelial cells that stream through the sheets and clusters of epithelioid cells.1-4 All three tumors can also be hypercellular with variable levels of nuclear pleomorphism, nucleolar prominence, and intranuclear inclusions. The abundant, oxyphilic/eosinophlilic cytoplasm of the fibrolamellar variant of HCC can appear particularly similar to the cells of epithelioid angiomyolipoma.
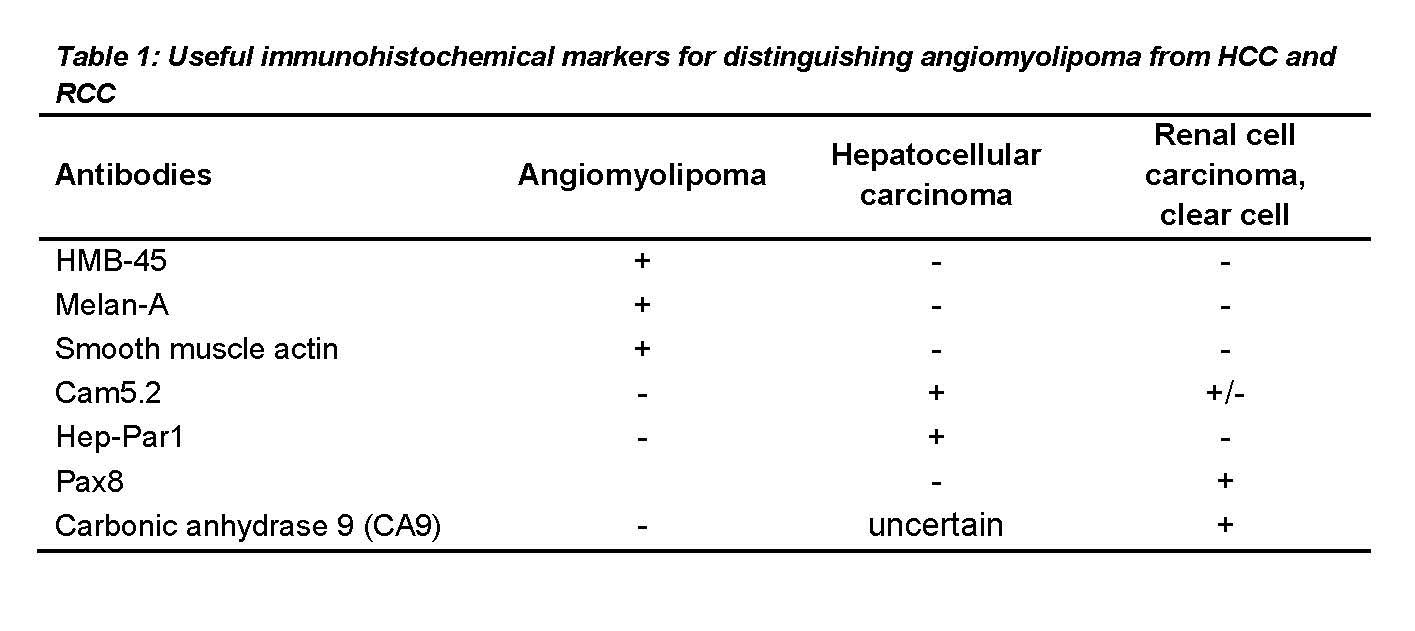
A few cytologic features can be helpful for distinguishing these tumors. Peripheral wrapping of endothelial cells around clusters or thickened trabeculae of cells are thought to be more specific for HCC compared to angiomyolipoma or RCC.2, 4 Furthermore, in contrast to the syncytyial appearance and fibrillary cytoplasm of the epithelioid cells of angiomyolipoma, the malignant hepatocytes of HCC have well-defined cytoplasmic borders and granular cytoplasm. Angiomyolipomas are often associated with extramedullary hematopoiesis, so the presence of hematopoietic elements in the aspirate may favor angiomyolipoma rather than HCC or RCC. Ultimately, immunohistochemistry plays a critical role in distinguishing these tumors (Table 1). Angiomyolipomas typically stain for melanocytic (HMB45, Melan-A) and myoid (smooth muscle actin) markers but do not show expression of cytokeratins, Hep-Par1, Pax8, and CA9.
In the current case, resection of the liver mass showed sheets of epithelioid cells with abundant eosinophilic cytoplasm (Figure 6). In areas, bile ductules entrapped within the sheets of tumor cells were present (Figure 7). In contrast to the trabecular architecture and densely granular and eosinophilic cytoplasm of normal hepatocytes, the tumor cells demonstrated a syncytial growth pattern and pale-pink, fibrillary cytoplasm (Figure 8). Tumor cells also showed perinuclear condensation of cytoplasm, leaving a web-like clearing around the cell periphery (Figures 5 and 8). Nuclei of the tumor cells were ovoid with prominent nucleoli.
Immunohistochemical stains for HMB45 (Figure 9) and smooth muscle actin (Figure 10) highlighted the tumor cells. Tumor cells showed no expression of Hep-Par1 (Figure 11). The overall morphology and immunophenotype were diagnostic of hepatic angiomyolipoma.
Angiomyolipomas are mesenchymal neoplasms that are composed of varying proportions of thick-walled vessels, smooth muscle, and fat. These tumors are classified in the family of perivascular epithelioid cell tumors (PEComas) that show dual immunophenotypic differentiation along the myocytic and melanocytic lineages. Other members of the PEComa family include lymphangioleiomyomatosis and clear cell (sugar) tumor of the lung. Angiomyolipomas are most commonly seen in the kidney, but extrarenal forms have been described in multiple organs, including the liver. Most cases of hepatic angiomyolipomas occur sporadically; approximately 6% arise in patients with tuberous sclerosis, due to mutations in the genes TSC1 (chromosome 9q34, encoding the hamartin protein) or TSC2 (chromosome 16p13.3, encoding the tuberin protein). Reports on the clinical features of hepatic angiomyolipoma vary, but several case series have described a wide age range (average ~50 years) and a female predominance. Hepatic angiomyolipomas may be discovered incidentally by imaging studies in asymptomatic patients; in others, presenting symptoms include abdominal pain, malaise, and anorexia.